Introduction
Phacoemulsification (phaco) is a type of cataract surgery technique that restores vision in patients whose lens are clouded. It is a process which utilizes an ultrasound device to remove the cataract. An intraocular lens (IOL) is then inserted.
The lens focuses light on the retina. The retina is located behind the cornea and is responsible for clear, sharp vision. It can change shape, also known as accommodation.
However, age causes the lens to harden and lose its ability to accommodate. The lens lies within a lens capsule. Due to age, dead cells emanating from an oxidative process can accumulate in the lens capsule. These cells cause the clouding of the lens to affect the clear, sharp vision. Cataracts can also be genetic or form due to smoking, injury, exposure to toxins and diseases like diabetics.
Phacoemulsification has significantly improved cataract surgery. Before, surgeons would remove the whole lens and capsule which made it difficult to fix the IOL. Because of the lens’ focusing ability, removing the cataract meant an individual ended up with an extreme case of farsightedness. To help these patients see after cataract surgery, surgeons recommended cataract glasses. These glasses were heavy, thick and magnified the eyes.
Due to improvements in technology, scientists have improved on IOLs by creating foldable IOLs that allow surgeons to make smaller incisions. The choice of which phaco technique to use depends on the density and size of the cataract.
Purpose
The purpose of phaco is to restore vision by removing the cloudy lens and replacing it with an IOL. With IOLs, patients experience a dramatic improvement in vision.
Preparation & expectation before Surgery
The surgeon will perform phacoemulsification from an outpatient surgical suite.
- Patients will need a complete physical examination to determine their state of health.
- Patients should not eat or drink anything several hours to the operation. Any ongoing medications should be declared and blood thinners should be stopped two weeks before surgery. They may be put on antibiotics before the surgery to minimize the chances of an infection.
- Patients will undergo an A-scan measurement to establish the eyeball’s length and the IOLs refractive power.
- Patients must make transport arrangements before the surgery.
Procedure
The following occurs in a phaco procedure:
- The eye is scrubbed before surgery and sterile drapes placed over the patient’s head and shoulders.
- The medical professional will administer antibiotics, steroids, non-steroidal inflammatory medications and dilating eye drops. The professional will inject local anesthesia on the lower eyelid to numb the eyeball.
- The surgeon will put a speculum over the eyelid to keep the eye open.
- Next, the surgeon will apply pressure on the eyeball using his/her hand to check if any bleeding has occurred as a result of anesthesia use. Applying pressure helps to stop the bleeding and to lower intraocular pressure (IOP).
- The surgeon will attach an oxygen tube to the patient to enable breathing since it’s difficult to breathe through the draping.
- Looking through a microscope, the surgeon will make a small incision at the edge of the cornea. An opening in the membrane surrounding the lens is created.
- After making the incision, the surgeon will inject in the eye viscoelastic fluid to reduce shock to the intraocular tissues.
- The surgeon will make a circular incision in the membrane surrounding the cataract.
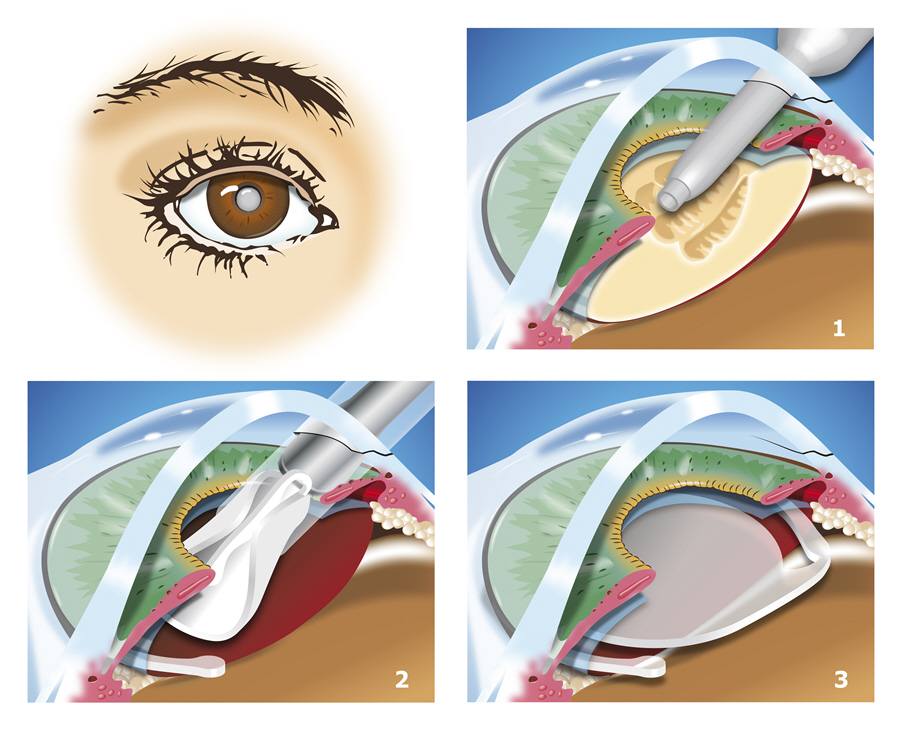
- A small ultrasonic probe which breaks up the cloudy lens into tiny pieces will be inserted. The vibrations from the instrument at ultrasonic speed chop off and almost dissolve the lens material into tiny fragments. The surgeon then suctions out the fragments from the capsule using an attachment on the probe tip. Both the lens and the front area of the capsule are removed. The posterior capsule is left intact to support the IOL.
- After removing the lens particle, the surgeon implants and positions an IOL into the lens’ natural capsule using an injector. He/she pushes the lens through where it unfolds and falls into position. The viscoelastic fluid is removed.
- The patient is required to wears protective glasses immediately after surgery.
After care, recovery, results
Most patients register improved vision almost immediately with vision steadily improving over a 4-5 week period. The incision the surgeon makes in the cornea heals on its own completely within a few days without stitches. Some patients may experience better color and depth perception. Some may no longer need lenses or glasses after surgery.
After surgery, the patient may need new corrective lenses for close vision.
The patient is required to visit the surgeon after 24 hours. Subsequently, they can go back to the surgeon after a week. The visits to follow can be made after three weeks then six to eight weeks after surgery.
The surgeon will prescribe eye drops which comprise of antibiotics, non-steroidal anti-inflammatory drugs and steroids to help prevent infection and reduce inflammation. The patient should take the antibiotic within seven to ten days.
The patient should wear a shield for protection while sleeping and avoid rubbing the eye. On the day following the operation, the surgeon removes the shield and recommends special tinted sunglasses.
Risks & complications
The following complications/risks may occur:
- Glaucoma
- Recurrent inflammation
- Blindness though very rare
- The IOL might get displaced
- Infections such as endophthalmitis (an infection in the eyeball)
- Development of a second cataract in the remaining area of the capsule
- An increase in floaters and flashes which could be a sign of retinal detachment
