Introduction
This is a surgical procedure that combines phacoemulsification (phaco) and canaloplasty (PCP).
Phaco is a cataract surgery done to restore clear vision where vision has turned cloudy from cataract formation. The procedure uses an ultrasonic device that breaks down (emulsifies) the cataract into smaller pieces, and then it is removed. After this, an artificial intraocular lens (IOL) is put inside the eye.
Cataract formation may be caused by injury to the eye, congenital developmental issues, disorders like diabetes and unprotected, prolonged exposure to sunlight. Older people are also at a higher risk of developing cataracts. Cataract surgery is one of the most widely recognized and safest surgeries in the world. Phaco is the most popular type of cataract surgery.
Canaloplasty is an advanced, minimally invasive, and non-penetrative surgical procedure used to manage open-angle glaucoma. The procedure helps to ease the drainage of aqueous humor by dilating Schlemm's canal. Aqueous humor is a fluid that's responsible for maintaining the eyes' intraocular pressure (IOP). When there is an accumulation of aqueous humor due to an obstruction in the drainage canal, IOP raises. Elevated IOP causes glaucoma.
Glaucoma causes irreversible vision loss and is one of the major causes of blindness in older people. It is considered a safer alternative to traditional glaucoma surgeries, such as trabeculectomy because it has a low complication rate.
By combining phaco and canaloplasty, the specialist can address both glaucoma and cataracts at the same time. These two surgeries work well together because canaloplasty is minimally invasive, meaning that the IOP will be lowered in the long term without sacrificing quick visual recovery. Cataract phaco can also lead to further intraocular pressure reduction.
Phacocanaloplasty has become a preferred method to treat both glaucoma and cataracts as both eye conditions are commonly seen in elderly patients. Because this combined surgery results in less trauma compared to when the two surgeries are done separately, phaco-canaloplasty is seen as a superior procedure.
Phaco-canaloplasty is effective in lowering the number of glaucoma medications the patient is using and increases the chances of lower IOP. A patient with a visually significant cataract and glaucomatous optic neuropathy is a strong candidate for the procedure. It is also suitable for patients with cataracts who use many medications.
Also Known As
- Phacoemulsification-canaloplasty
Before the Procedure
Before the surgery commences, the specialist will conduct a comprehensive eye examination, including IOP check, visual acuity, check corneal curvature, and imaging tests. The specialist may also conduct physical checks such as MRI, chest x-rays, ECG, and routine blood tests.
The specialist will also ask for the patient's medical and surgical history. The patient must disclose all the medical conditions they suffer from and all medication they take. Before the surgery day, the surgeon will discuss the most suitable type of IOL the patient needs.
The surgeon prescribes antibiotic eye drops to use before the surgery to help minimize the risk of infection. The patient is advised to stop taking blood thinners and stop smoking a few days to the surgery. Patients suffering from diabetes and hypertension will receive specific instructions on how to use their medication from the specialist.
Due to the use of local anesthesia, the patient will be asked to fast a few hours to the surgery or have a very light breakfast on the morning of the surgery. They are also asked not to drive home as their vision will be affected for a few hours.
Procedure
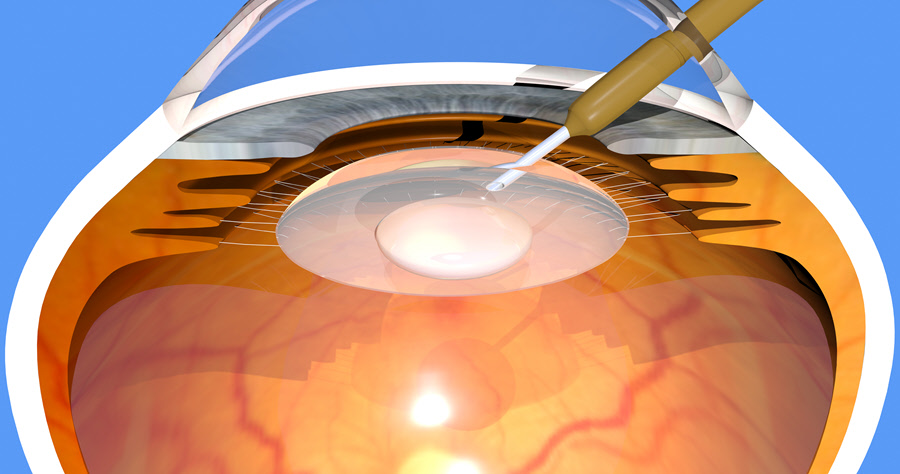
Phaco is done first. First, the patient is put under local anesthesia. The surgeon can also decide to sedate the patient. A speculum is used to keep the eye open. Once the anesthesia or sedation takes effect, the surgeon looks through a microscope and makes a small incision on the side of the anesthetized cornea and makes a hole in the lens membrane. The incision site depends on the cataract's size and denseness.
The surgeon then inserts an ultrasonic handpiece with a phaco needle (a small, titanium/steel needle) into the cornea. The tip vibrates and emits ultrasonic waves that slowly break down (emulsify) the cataract. An attached pump simultaneously suctions the fragments out of the capsule, while leaving the posterior capsule intact. The surgeon then implants the IOL into the remaining capsule.
This process takes about 20 minutes. Once phaco is done, canaloplasty follows after.
The specialist creates a parabolic scleral flap about half as the sclera's thickness. S/he creates another incision to give access to Schlemm's canal. After unroofing Schlemm's canal, a flexible microcatheter is pushed forward through the canal. As the microcatheter advances, a viscoelastic fluid is introduced into the canal to dilate it.
Once the microcatheter goes through the canal's entire 360 degrees, it is removed while a suture is threaded. The suture is tied down, creating tension, which makes the canal's walls stretch open for a long time. As the suture is tied down, the microcatheter is slowly removed in the opposite direction. The suture now replaces the microcatheter. The suture is knotted to distend the trabecular meshwork inwardly and keep Schlemm's canal open. The scleral flap is then repositioned and closed tightly. The eye is dressed and an eye shield placed to prevent injury.
Risks & Complications
Some complications that may occur include:
- Mild hyphema
- Corneal edema
- Astigmatism
- Endophthalmitis
- IOL dislocation
- Retinal detachment
- Hypotony
- Surgery failure
Aftercare & Recovery
The patient will be given steroid and antibiotic eye drops to use for two weeks postoperatively. If they experience any mild pain, they can take some over-the-counter pain medication. They will also be required to keep wearing the eye patch for a while to avoid harming the eye.
During the healing period, the patient should avoid:
- Rubbing the eye
- Getting water into the eye
- Using eye-makeup
- Contact sports and strenuous tasks
There will be follow-up visits after one day, two weeks and one, three, six and 12 months postoperatively. There are no dietary instructions that the patient will be required to follow after the surgery. The patient can resume their activities a few days later.
Outcome
If the postoperative IOP doesn't lower by 20% or remains higher than 21mmHg, the surgery is considered as unsuccessful.
