Introduction
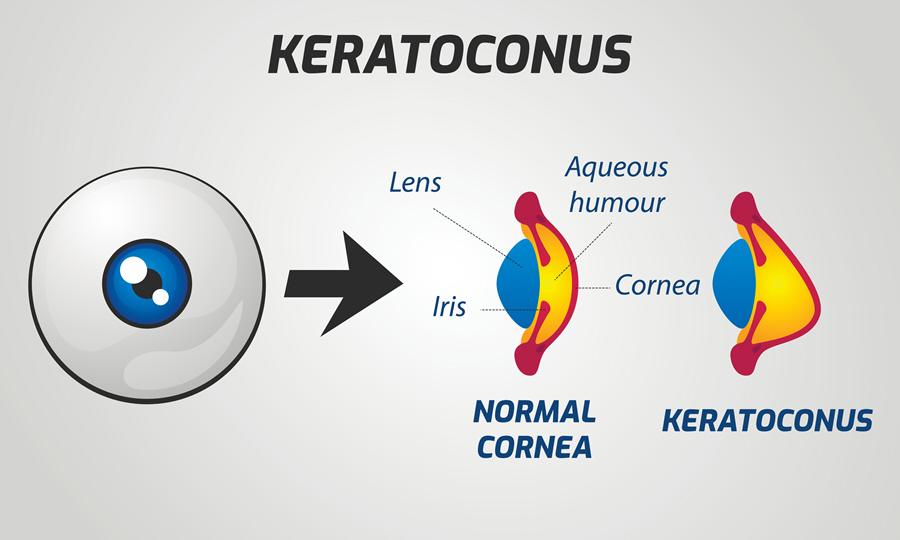
Keratoconus is dystrophy that involves the structure of the cornea. It occurs when the cornea becomes thin and forms a cone-like bulge. The cornea is the transparent, dome-shaped tissue that covers the front of the eye. Changes in the shape of the cornea cause light rays to stay out of focus leading to blurry and distorted vision. Keratoconus makes daily tasks such as driving or reading difficult.
Keratoconus usually begins manifesting itself in people between the age of 10 and 25. Vision deteriorates in a 10-20 year period. For some people though, vision can suddenly decrease when the cornea bulges unexpectedly. The cornea may also start to scar causing it to lose its smoothness and become less clear. This leads to a more distorted and blurry vision.
Also Known As
- KC
- KCN
- Conical Cornea
- Vision changes - keratoconus
- Noninflammatory corneal thinning
Sub-Types
Causes and Risk Factors
The cause of Keratoconus is unknown. However, it is thought to be genetic and present at birth. It may also be due to a defect in collagen, a tissue that provides shape and strength to the cornea. Risk factors include:
- Down syndrome
- Lax eyelids
- Vigorously rubbing the eyes
- Obstructive sleep apnea
- A family member with keratoconus
- Atopy where an individual tends to develop many allergies
- People with a history of myopia (nearsightedness). As myopia gets worse, astigmatism develops and worsens over time
- Certain connective tissue disorders such as osteogenesis imperfecta, Ehlers-Danlos syndrome and Marfan syndrome
- Congenital disorders which also cause poor vision such as Leber congenital amaurosis, lack of an iris and retinopathy of prematurity
Signs & Symptoms
Keratoconus usually affects both eyes. However, each eye may experience vision differently. The symptoms also do not remain static; they can change over time. During the early stages of Keratoconus, one may experience the following symptoms:
- Swelling
- Red eyes
- Mild blurring of vision
- Glare and increased sensitivity to light
- Straight lines look bent leading to a slightly distorted vision
During later stages, the symptoms may include:
- Vision that cannot be corrected by eyeglasses
- Worse blurry and distorted vision
- Increased astigmatism (the eye does not focus as it should) leading to frequent new eyeglass prescriptions
- Increased myopia (nearsightedness)
- Discomfort in wearing contact lenses since they may no longer fit properly
Diagnosis
The eye care professional can detect keratoconus through a routine eye examination. He/she will also do the following:
- Corneal topography where he/she will map the eye to reveal the condition of the cornea’s surface
- Use a slit-lamp examination to detect the disease in its later stages
- Examine the cornea and measure its curve. This will reveal any changes in the cornea’s shape
- Pachymetry to measure the thickness of the cornea
Treatment
Treatment of Keratoconus aims to provide functional visual acuity and stop the progression of the disease.
Medical Treatment
Treatment for Keratoconus depends on whether the symptoms are mild or severe. Keratoconus with mild vision can initially be corrected with eyeglasses or soft contact lenses. Due to the progression of the disease, a patient will need to wear rigid gas-permeable contact lenses, hybrid sclera or other types. Contact lenses assist in keeping the vision in proper focus. The lenses only provide vision but do not treat or stop the progression of the disease.
Surgical Treatment
For many years, the only cure for keratoconus was a corneal transplant. However, newer methods to treat the disease have been unveiled.
Keratoconus can now be treated using corneal implants such as Intacs or intracorneal ring segments in mild to moderate patients. The surgeon will insert Intacs (a small curved device) in the cornea. Intacs flatten the cornea’s curve. Contact lenses will also fit better after this procedure.
High-frequency radio energy (conductive keratoplasty) can be used to alter the cornea’s shape to enable the contact lenses to fit better.
The surgeon can do collagen cross-linking (use of a special UV light and eye drops) to strengthen, flatten or stiffen the cornea. This procedure keeps the cornea from bulging and getting worse. A laser is then used to reshape the cornea.
Deep anterior lamellar keratoplasty involves transplanting only the front and middle layers of the cornea. Patients tend to heal faster and suffer less risk of rejection.
If acute corneal fluid (hydrops) develops or the cornea becomes too thin as to affect vision severely, a corneal transplant is necessary. All parts of the diseased cornea are replaced with healthy corneal tissue from a donor.
Home Care
The patient should never rub the eye. Rubbing the eye can damage corneal tissue and worsen the symptoms. Itchy eyes are best treated with medicines prescribed by the doctor.
Prognosis/Long-term outlook
Untreated keratoconus may lead to so much thinning of the cornea that a hole develops in the thinnest part worsening vision.
It is possible for the new cornea to be rejected after a transplant. This risk, however, is lower compared to other organ transplants.
In most cases, rigid gas-permeable contact lenses will correct vision. The cornea also becomes stable after a few years and does not cause severe problems with vision.
In the event of a corneal transplant, the prognosis is often excellent. However, a patient may take longer to recover and may still need eyeglasses or contact lenses.
People with keratoconus should not have laser vision correction such as LASIK. However, Photorefractive keratectomy (PRK) may be safe for people with mild keratoconus and who have had collagen cross-linking.
All surgical patients will need close follow-up to complete rehabilitation.
Prevention/Follow Up
There is no known or proven prevention for keratoconus. Some people, however, feel that avoiding allergens and rubbing the eye can help prevent the disease.
