Introduction
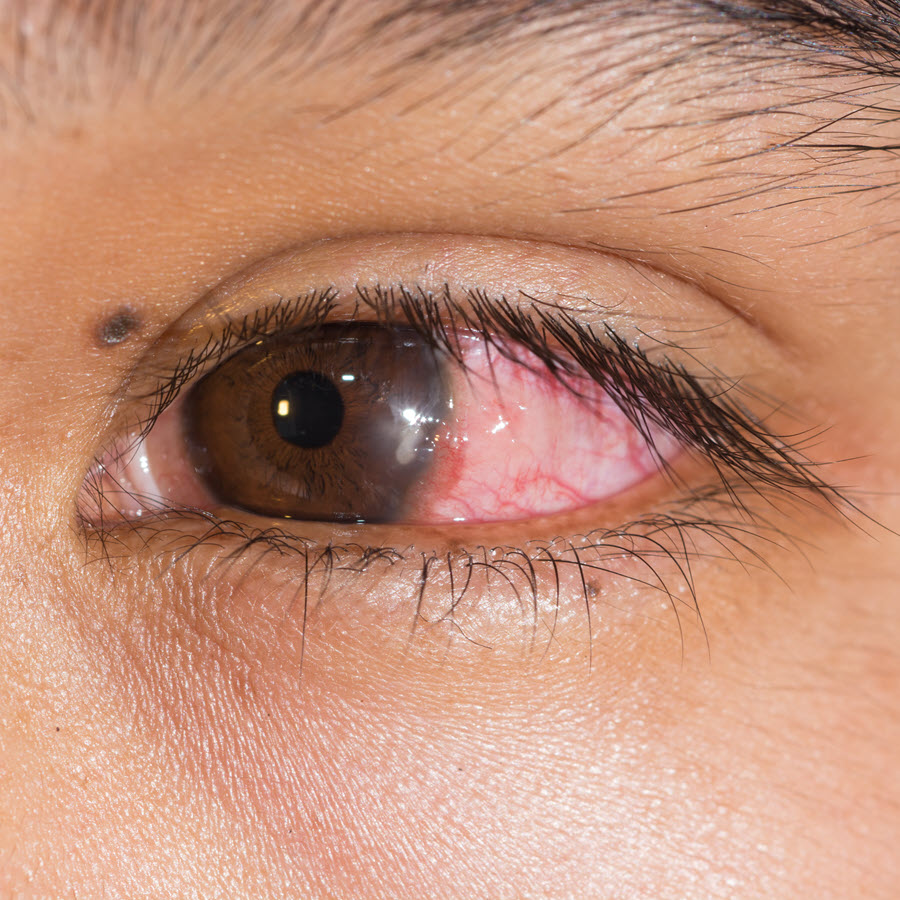
Bacterial keratitis refers to an infection in the cornea. The cornea is the transparent dome-shaped covering at the front of the eye. Bacterial keratitis is serious because it can cause blindness within 24-48 hours.
Various types of bacteria cause bacterial keratitis. However, two of these bacteria are responsible. They include staphylococcus aureus and pseudomonas aeruginosa. Pseudomonas bacteria live in water and soil. Staphylococcus aureus bacteria are found on human skin. They can also be located on the mucous membrane (a protective lining inside the body). Bacterial keratitis is not infectious.
Also Known As
Bacterial corneal ulcer
Causes and Risk Factors
Bacteria are responsible for bacterial keratitis. Risk factors include:
- Wearing contact lenses - Those with extended-wear contact lenses are most at risk. Other issues related with contact lenses may include:
a) Overnight wear
b) The cornea being re-shaped using rigid contact lenses
c) Poor disinfection of contacts
d) Failing to clean the cases
e) Rinsing and storing contacts in water
f) Using infected lens solution
g) Reusing contact lens solution
- Problems with the eyelids or tearing
- Weakened or compromised immune system
- Ocular trauma (thermal injuries, chemicals and foreign bodies)
- Loose sutures from surgery
- Recent corneal diseases such as herpetic keratitis, chronic corneal diseases like dry eyes
- Ocular surface diseases such as chronic epithelial defect, corneal exposure, aqueous tear deficiency and so on
- Topical corticosteroids used to treat eye disorders
- Corneal edema (accumulation of fluids)
Signs & Symptoms
The following symptoms may be present:
- Difficulty seeing or reduced vision
- Pain, usually sudden
- Photophobia
- Discharge from the eyes
- Excessive tearing
Diagnosis
Using a slit lamp (an instrument with high magnification), the eye professional will check for:
- Epithelial defects usually seen after applying fluorescein (a dye)
- Best corrected visual acuity
- Corneal infiltrates (whitish opacities)
- A thinning cornea or corneal edema
- The cells, hypopyon, fibrin and flare of the anterior chamber
The professional will conduct a seidel test to check if the aqueous humor is leaking.
He/she may do a culture of corneal tissue, contact lens cases, eye solutions and so on. If the eye shows no improvement after a culture, a corneal biopsy may be considered.
Slit lamp photography in chronic, unresponsive cases may be undertaken. A B-scan ultrasound is ideal for severe cases of corneal ulcer. The professional will also check for intraocular pressure.
Treatment
Treatment of bacterial keratitis aims to clear the bacterial infection from the eye.
Medical Treatment
Patients will have to remove the contact lenses.
Bacterial keratitis is often treated with frequent topical antibiotic drops. Steroids may also be used. Oral antibiotics should be considered for patients with sclera movement or deep ulcers. Pain medications may be prescribed according to need.
Surgical Treatment
If medical treatment fails, a corneal transplant may be considered. A transplant procedure involves the patient receiving a cornea from a donor.
Prognosis/Long-term outlook
If bacterial keratitis is not treated promptly, it may lead to sight-threatening complications such as perforation, sclera extension and corneal scarring. It may also lead to anterior segment disorganization, chronic corneal inflammation and endophthalmitis. Ultimately, bacterial keratitis may lead to blindness. In some cases, even transplants may not work leading to permanent vision impairment.
The patient will need to return to the doctor several times for close monitoring. Severe cases are monitored daily while non-severe ones can be monitored less frequently. In severe non-responsive cases, hospitalization may be considered.
Prevention/Follow Up
- Since the majority of infections come from contact lens wear, it’s imperative that individuals take great care. The following will help keep bacteria away from the eyes:
- Following the eye care provider's instructions to the letter
- Washing of hands with soap and water. The hands should be dried with a lint-free towel before the lenses are handled
- Keeping the contact lenses away from water, hot tubs, swimming pool water and so on
- Not rinsing or storing the contacts in tap or non-sterile water
- Refusing to wet the lenses using saliva (saliva contains bacteria)
- Avoiding use of saline solution and rewetting drops to disinfect lenses
- Ensuring that one never sleeps in contact lenses
- Wearing the contact lenses strictly according to the eye care professional's schedule
- Rubbing and rinsing the contact lenses as a way of cleaning them. The lenses should be rubbed with the fingers and rinsed in the lens solution
- Rinsing the contact lens case using fresh solution as opposed to water. The empty case should be left open to dry.
- Keeping the case housing the contact lens clean. The case should be replaced regularly, at least after three months. Cracked or damaged contact lens cases should be avoided.
- Avoiding “topping off” or re-using the solution inside the lens case.
- Refusing to transfer the contact lens solution into another container
- Keeping the tip of the solution bottle from touching any surface. The bottle should be tightly closed when not in use.
- Taking care to not wear the lenses after storing them for 30 or more days without disinfection
- Sharing contact lenses for cosmetic purposes is not advisable
Individuals should also use protective eyewear for sports and outdoor activities
